Vaccination success for rural Victoria.
I (like most of you) have been at times overwhelmed by the infodemic of COVID and vaccination information that has been flooding our inboxes and Twitter feeds.
I’m always interested to understand the level of equity in health programs. My post from the early days provided an illustration of how in the (very) early days - COVID-19 was an illness of the rich. Wow, how that changed over time.
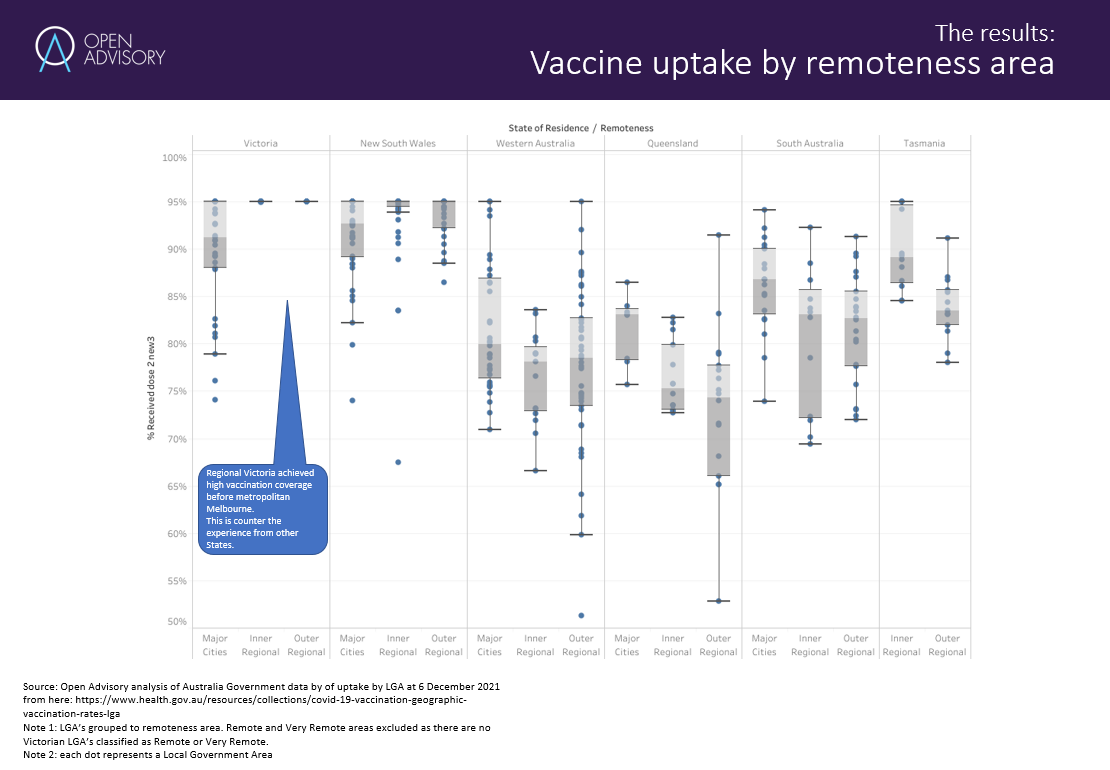
For a current engagement, I was trying to reproduce this analysis of vaccine uptake by remoteness area across Australia, neatly showing the high uptake in rural Victoria.
I get a similar result using the weekly data published by the Australian Government. Here’s my version:
I haven’t however seen an analysis of the uptake by communities when controlling for levels of socioeconomic disadvantage.
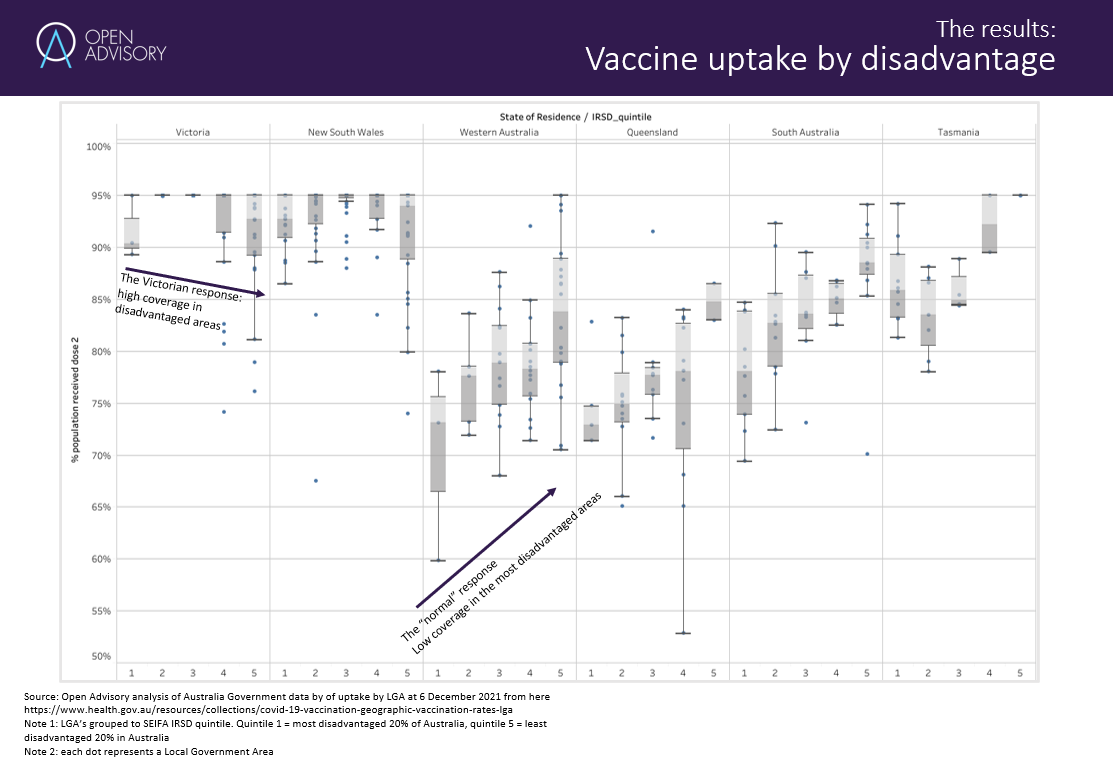
Grouping the Local Government Areas to SEIFA quintiles of the Index of Relative Socioeconomic Disadvantage (IRSD) provided an amazing illustration of the equity in the vaccine uptake in Victoria.
Other States had the “typical” outcome of low coverage in the most disadvantaged areas - but Victoria had the highest coverage in disadvantaged areas.
So what comes next?
Is this now a template for other public health programs? What are the program design lessons we can all use?